Ovarian Water Cyst in Females: Causes, Pregnancy Complications, Home Remedies, Prevention & Complete Treatment Guide 2026
Written By: Maria Kanwal Written and Reviewd In May 2026
You’re not the only person who has lately been informed that you have a “water cyst” on your ovary. Every year, millions of women are diagnosed with ovarian cysts, the great majority of which are benign sacs filled with fluid. But what happens if these cysts develop during pregnancy, get bigger, or last longer? At that point, comprehending them becomes really important.
Every query women have on the internet is addressed in this thorough guide: What is an ovarian water cyst? How is it formed? Can it be brought on by early dietary or lifestyle choices? Is it risky when pregnant? Above all, how do you prevent it, cure it, and safeguard your reproductive health?
What Is an Ovarian Water Cyst? (Simple Ovarian Cyst Explained)
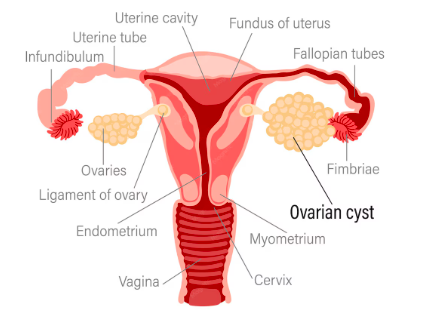
A thin-walled, fluid-filled sac that develops on or inside the ovary is known medically as an ovarian water cyst — also called a simple cyst, serous cyst, or functional cyst. A water cyst appears as a smooth, dark pocket on an ultrasound scan because it is completely filled with a clear, watery fluid (serous fluid), in contrast to complicated cysts, which may contain solid components or internal walls.
In women of reproductive age, these cysts are the most prevalent kind of ovarian cyst. Simple, smooth ovarian cysts smaller than 3 cm that appear to be filled with water are regarded as a typical aspect of ovarian function, according to research published in Cureus (2025).
Key Statistics at a Glance
• The majority of women of reproductive age naturally develop small cysts every month
• Approximately 8% of premenopausal women develop large, problem-causing cysts
• Ovarian cysts are present in approximately 16% of postmenopausal women
• Ovarian cysts during pregnancy: estimated at 0.2%–2% of all pregnancies
Serous Ovarian Cyst — A Closer Look
A serous ovarian cyst (serous cystadenoma) is one of the most common benign ovarian tumors. It is lined by cells that resemble the fallopian tube epithelium and filled with thin, watery (serous) fluid — hence the name. Serous cystadenomas are almost always unilateral (affecting one ovary), grow slowly, and can reach 5–15 cm. They appear on ultrasound as smooth, thin-walled, single-chambered cysts. While the overwhelming majority are benign, a serous borderline tumor or serous carcinoma can occasionally develop from these cells — making routine monitoring essential once a serous cyst is diagnosed.
Serous cysts account for roughly 20–25% of all ovarian cysts and are most commonly found in women aged 20–50. Unlike functional cysts, they do not disappear on their own and typically require surgical removal if they grow beyond 5–7 cm or cause symptoms.
Follicular Cyst of the Ovary — What Every Woman Should Know
A follicular cyst is the most common type of ovarian water cyst and the one most frequently found in women of reproductive age. It forms when a dominant follicle — the sac that contains a developing egg — fails to rupture at ovulation. Instead of releasing the egg and collapsing, the follicle continues to fill with fluid, growing into a cyst that can reach 2–10 cm in diameter.
The good news: follicular cysts are almost always benign and self-limiting. Most resolve naturally within one to three menstrual cycles without any medical intervention. However, a follicular cyst that grows larger than 5 cm, causes significant pelvic pain, or fails to resolve within 3 months warrants closer monitoring and possible treatment.
Follicular Cyst Quick Facts
• Cause: Ovulation failure — follicle doesn’t rupture
• Size: Typically 2–10 cm
• Resolution: Most resolve in 1–3 menstrual cycles without treatment
• Risk: Torsion or rupture if >5–6 cm
• Treatment: Watchful waiting; hormonal therapy to prevent recurrence
Other Types of Ovarian Cysts (Water-Filled)
Not all ovarian cysts are the same. Your risk level and treatment path are determined by the type:
- Corpus Luteum Cyst: Forms after ovulation when the follicular sac does not shrink properly. Can grow up to 10 cm and may cause bleeding.
- Para-ovarian Cyst: A simple cyst formed from remnants of embryonic tissue, located beside the ovary. Does not disappear on its own.
- Endometrioma: When endometrial tissue grows on the ovary; frequently called a ‘chocolate cyst’ due to its dark fluid content.
- Theca-Lutein Cysts: Associated with elevated hCG hormone levels, often seen in multiple pregnancies or gestational conditions.
How Does an Ovarian Water Cyst Form?
Women are better able to identify risk factors early when they understand the formation process. Every month, the ovaries produce follicles — tiny fluid-filled sacs that each contain an egg. Normally, one follicle grows dominant, ruptures to release its egg at ovulation, and the remaining sac (corpus luteum) dissolves. When this process breaks down, fluid accumulates and a cyst forms:
- Ovulation failure: The dominant follicle does not rupture, continues growing, and becomes a follicular cyst.
- Corpus luteum persistence: After ovulation, the collapsed follicle fills with blood or fluid instead of reabsorbing.
- Hormonal disruption: Imbalances in estrogen, progesterone, FSH, or LH interfere with the normal ovulatory cycle.
- Endometrial implantation: Endometrial tissue implants on the ovary and bleeds cyclically, forming cysts.
- Epithelial cell growth: Surface cells of the ovary grow inward, fill with fluid, and form inclusion cysts.
- Excessive hCG stimulation: Seen in pregnancy or IVF treatment, causing theca-lutein cysts in both ovaries.
Ovarian Cyst Causes in Young Girls & Early Life Risk Factors
One of the most searched questions online is: ‘Why did I develop an ovarian cyst at such a young age?’ The answer lies in a combination of hormonal, dietary, and environmental factors that begin influencing ovarian health from puberty onward. Research confirms that benign ovarian cysts are found in approximately 68% of ovaries in girls aged 2–12 years, with most being tiny and resolving naturally. However, the habits formed in early life can create a cumulative risk that manifests in the reproductive years.
Which Foods & Activities in Early Life Can Trigger Ovarian Cysts?
Emerging research strongly suggests that dietary habits, physical activity levels, and lifestyle choices — especially during adolescence and early adulthood — play a significant role in ovarian health:
Foods Associated with Higher Ovarian Cyst Risk
- Red & Processed Meat: Studies show women who consume high amounts of beef, pork, and processed meats have a significantly higher risk of seromucinous ovarian cysts. One case-control study found an odds ratio of 2.7 for high beef consumption.
- Refined Sugar & High-Glycemic Foods: Sugar triggers insulin spikes that directly promote androgen excess and cyst formation — especially harmful for young women with early insulin resistance or PCOS.
- Trans Fats & Fried Foods: French fries, chips, and fried items increase inflammatory markers and worsen insulin sensitivity, creating a hormonal environment where cysts thrive.
- High-Fat Dairy Products: Full-fat dairy may influence estrogen metabolism in some women, contributing to hormonal imbalance.
- Alcohol & Excessive Caffeine: Both disrupt hormonal balance and stress the liver — the organ responsible for metabolizing excess hormones.
Lifestyle Habits in Early Life That Raise Risk
- Sedentary lifestyle: Linked to higher BMI, insulin resistance, and hormonal imbalance — all cyst risk factors.
- Chronic stress: Elevates cortisol, disrupting the hypothalamic-pituitary-ovarian axis and interfering with normal ovulation.
- Poor sleep: Disrupts hormonal regulation, particularly estrogen, progesterone, and melatonin cycles.
- Early onset of menstruation without nutritional guidance: Young girls are more vulnerable without adequate dietary support.
- Exposure to environmental estrogens (xenoestrogens): Found in plastics, pesticides, and some personal care products — these mimic estrogen in the body.
- Use of fertility medications: Drugs that stimulate ovulation may increase the risk of developing cysts as a side effect.
Ovarian Cyst Symptoms in Women — What to Watch For
Many ovarian water cysts produce no symptoms at all and are discovered incidentally during a routine pelvic ultrasound. When symptoms do appear, they include:
- Dull, aching pelvic pain — usually on one side (the side of the cyst)
- Bloating or a sensation of fullness in the lower abdomen
- Irregular or painful menstrual periods
- Pain during sexual intercourse
- Frequent urination or difficulty fully emptying the bladder
- Difficulty getting pregnant — particularly in cases of PCOS or endometriomas
- Sudden, sharp pelvic pain — this could signal rupture or torsion requiring emergency care
- Nausea and vomiting if the cyst causes ovarian torsion
Emergency Warning Signs — Seek Immediate Medical Care
Sudden severe abdominal pain accompanied by nausea, vomiting, fever, or dizziness may indicate a ruptured cyst or ovarian torsion. These are medical emergencies requiring immediate hospital attention.
Ovarian Water Cysts & Pregnancy: Risks, Complications & What to Expect
One of the most searched topics online is: ‘Can I get pregnant with an ovarian cyst?’ and ‘What happens if a cyst is found during pregnancy?’ Here is the full, evidence-based picture.
Ovarian Cyst and Fertility Problems — Can Cysts Stop You from Conceiving?
Most ovarian cysts do not prevent pregnancy. Simple functional cysts generally resolve on their own and have no impact on fertility. However, certain types — particularly those associated with endometriosis or PCOS — can interfere with ovulation, create hormonal imbalances, or damage the fallopian tubes structurally, making conception more challenging.
For women facing difficulty conceiving due to ovarian cysts, early diagnosis and targeted medical intervention can significantly improve fertility outcomes. Treatments include hormonal therapy, lifestyle modifications, laparoscopic surgery, or assisted reproductive techniques like IVF depending on severity.
Ovarian Cyst in Early Pregnancy — What Happens in the First Trimester?
Discovering an ovarian cyst in early pregnancy is more common than most women realize. Due to the widespread use of early ultrasound screening, cysts are now identified in 0.2%–2% of all pregnancies, often during the first prenatal scan.
During the first trimester, the corpus luteum — the sac that remains after ovulation — is essential for producing progesterone to sustain the pregnancy. This corpus luteum cyst can grow to 5–6 cm and often appears alarming on ultrasound. The reassuring news: these cysts almost always resolve naturally by weeks 12–16 as the placenta takes over progesterone production. Routine monitoring is sufficient in most cases.
First Trimester Ovarian Cyst — Key Facts
• Corpus luteum cysts in early pregnancy are normal and expected
• Most resolve by weeks 12–16 of gestation without treatment
• Cysts persisting beyond 16 weeks are typically non-functional and require monitoring
• 65–80% of persistent cysts are asymptomatic and continue until after delivery
Simple Ovarian Cyst During Pregnancy — Is It Dangerous?
A simple ovarian cyst found during pregnancy — one that is smooth, thin-walled, fluid-filled, and under 5 cm — is generally not dangerous. Research published in a Journal of Obstetrics and Gynecology case series confirmed that the majority of pregnancy-related cysts are simple or functional, with most managed conservatively without complications.
However, ‘simple’ does not mean ‘ignore.’ Even simple cysts require periodic ultrasound monitoring to ensure they are not growing, as size increase changes the risk profile significantly.
Ovarian Cyst Pain During Pregnancy — Understanding the Discomfort
Pelvic pain is one of the most alarming symptoms for pregnant women with known ovarian cysts. Understanding the difference between normal discomfort and warning signs is critical:
- Mild, one-sided dull aching or pressure: Often normal, especially from a corpus luteum cyst supporting early pregnancy. Monitor and report to your doctor.
- Pain that worsens with position changes or physical activity: Could indicate the cyst is enlarging or at risk of torsion. Seek prompt evaluation.
- Sudden, severe, sharp pain: A potential emergency — may signal cyst rupture or ovarian torsion. Go to the emergency room immediately.
- Pain accompanied by fever, vomiting, or shoulder tip pain: These are serious signs requiring immediate hospital care.
Ovarian Cyst Rupture During Pregnancy — What to Know
An ovarian cyst rupture during pregnancy occurs when the expanding uterus compresses an existing cyst, causing it to burst. This is a serious complication that can result in:
- Severe acute abdominal pain — sudden onset, often on one side
- Internal hemorrhage — bleeding into the abdominal cavity
- Drop in blood pressure and signs of shock in severe cases
- Threat to both maternal and fetal well-being in cases of significant hemorrhage
Smaller cysts may rupture with minimal bleeding and can sometimes be managed conservatively. Larger cyst ruptures often require surgical intervention. Any sudden, severe pain during pregnancy must be evaluated immediately — do not wait to ‘see if it passes.’
Ovarian Torsion in Pregnancy — A Surgical Emergency
Ovarian torsion during pregnancy occurs when an ovarian cyst displaces the ovary, causing it to twist on the ligament supporting it. This cuts off blood supply to the ovary and is one of the most urgent gynecological emergencies in pregnancy. Symptoms include:
- Sudden, severe, one-sided pelvic or lower abdominal pain
- Nausea and vomiting — often severe
- Fever in later stages as tissue begins to die
- The pain may come in waves initially, then become constant
Ovarian torsion requires emergency laparoscopic surgery to untwist the ovary and, if possible, preserve ovarian function. Delay in treatment can result in permanent loss of the ovary. The 2025 Indian obstetric case series documented ovarian torsion as the most urgent complication among women with cysts during pregnancy.
Is an Ovarian Cyst Dangerous During Pregnancy? — The Full Risk Picture
Documented Pregnancy Complications from Ovarian Cysts
1. Ovarian Torsion — Surgical emergency requiring immediate laparoscopy to preserve the ovary.
2. Cyst Rupture — Causes acute pain and potential internal bleeding threatening mother and fetus.
3. Obstructed Labor — Large pelvic cysts can block the birth canal, necessitating Caesarean delivery.
4. Fetal Malpresentation — Large cysts prevent the baby from moving into a head-down position.
5. Cyst Infection — Rare, but requires antibiotic treatment during pregnancy.
6. IUGR (Intrauterine Growth Restriction) — Documented in cases of giant cysts competing for abdominal space (2025 Journal of Surgical Case Reports: 35 cm cyst, 11 liters of fluid).
Can an Ovarian Cyst Cause Miscarriage?
While most ovarian cysts do not directly cause miscarriage, large or complex cysts — particularly those causing significant hormonal imbalances — can increase miscarriage risk in some women. Cysts associated with PCOS or endometriosis carry a higher indirect risk due to the underlying hormonal disruption these conditions create. Regular monitoring during pregnancy is essential to assess and manage any potential risks from existing cysts.
Ovarian Cyst Removal During Pregnancy — When and How
Ovarian cyst removal during pregnancy is considered when cysts are large (typically >5–6 cm), rapidly growing, symptomatic, or when there is concern about malignancy. The optimal timing and approach:
- Best timing: Second trimester (weeks 14–20) — lowest risk of pregnancy loss; uterus not yet too large to impede surgery.
- Preferred method: Laparoscopic cystectomy (keyhole surgery) — minimal invasiveness, fastest recovery, lowest fetal risk.
- Open surgery (laparotomy): Required for very large or complex cysts, or when laparoscopy is not feasible.
- Simultaneous Caesarean cystectomy: Performed at delivery when a large cyst has been monitored throughout pregnancy.
- Expectant management: Continued monitoring for stable, small, asymptomatic cysts with no malignant features.
How Is an Ovarian Water Cyst Diagnosed?
If you suspect an ovarian cyst or have been told you might have one, these are the standard diagnostic procedures:
- Pelvic Ultrasound: The gold standard. A simple cyst appears as a smooth, thin-walled, fluid-filled sac. Transvaginal ultrasound provides the clearest images.
- CA-125 Blood Test: A protein marker elevated in some ovarian cysts and cancers. Used cautiously as it can be elevated during pregnancy, endometriosis, and other benign conditions.
- MRI or CT Scan: Reserved for complex or ambiguous cases where ultrasound is inconclusive.
- Laparoscopy: A minor surgical procedure allowing direct visualization and potential removal of the cyst.
- Hormone Panel Blood Tests: To check FSH, LH, estrogen, progesterone, and androgens to identify underlying hormonal causes.
Ovarian Cyst Treatment Options — From Watchful Waiting to Surgery
Treatment depends on cyst size, type, growth pattern, your age, symptoms, and whether you are pregnant or trying to conceive.
1. Watchful Waiting (Expectant Management)
The most popular initial approach for simple, small cysts (under 5 cm) in reproductive-age women. Most functional cysts resolve naturally within 1–3 menstrual cycles. Your doctor will schedule follow-up ultrasounds every 4–6 weeks.
2. Pain Management
Over-the-counter medications like ibuprofen or paracetamol relieve mild pelvic pain while the cyst resolves naturally. Heat therapy — a warm pad on the lower abdomen — provides comfort for many women.
3. Hormonal Therapy (Ovarian Cyst Treatment Without Surgery)
Birth control pills (oral contraceptives) are prescribed to suppress ovulation and prevent new functional cysts from forming. They do not shrink existing cysts but significantly reduce recurrence. This is a key non-surgical treatment option for women with repeated functional cysts. Other hormonal options may include progesterone-only therapy in specific cases.
4. Functional Ovarian Cyst Treatment — What Works Best
Functional cysts (follicular and corpus luteum) are the most common and most treatable. The treatment algorithm is straightforward:
- Cysts under 5 cm with no symptoms: Watchful waiting with repeat ultrasound in 6–8 weeks.
- Cysts 5–10 cm or symptomatic: Hormonal suppression to prevent new cysts; monitor existing one.
- Cysts over 10 cm or persisting beyond 3 months: Laparoscopic cystectomy recommended.
- Cysts with complex features (solid areas, septations, blood flow): Surgical evaluation and possible biopsy.
5. Laparoscopic Surgery (Cystectomy)
Surgery is recommended when the cyst is large (typically over 10 cm), persistent, causing significant pain, or when malignancy is suspected. Laparoscopic cystectomy is minimally invasive, preserving the ovary and fertility in most cases. Recovery is typically 1–2 weeks.
6. Open Surgery (Laparotomy)
Required for very large or complex cysts — as illustrated by a 2025 Cureus case report in which a giant ovarian cyst necessitated an open surgical approach. The healthy ovary was successfully preserved in that case.
7. Oophorectomy (Ovary Removal)
In rare cases — particularly when cancer is suspected or when the cyst cannot be safely separated from the ovary — the ovary itself may be removed. Postmenopausal women with suspicious cysts may undergo bilateral salpingo-oophorectomy as a precaution.
8. Aspiration
Ultrasound-guided needle aspiration of cyst fluid is occasionally performed for simple cysts in specific clinical situations, though cysts may recur without treating the underlying cause.
Ovarian Cyst Diet Plan — Best Foods to Eat and Foods to Avoid
While diet alone cannot cure ovarian cysts, research clearly links certain nutritional patterns with either worsening or improving ovarian health. Here is the complete dietary guide:
Best Foods for Ovarian Health
Foods That Support Ovarian Health
- High-Fiber Foods: Whole grains (oats, quinoa, brown rice), lentils, pears, oranges, and legumes. Fiber helps balance estrogen levels by preventing re-absorption in the gut.
- Anti-Inflammatory Foods: Fatty fish (salmon, mackerel), turmeric, ginger, olive oil, and dark leafy greens reduce the chronic inflammation that promotes cyst growth.
- Healthy Fats: Avocados, nuts, seeds, and flaxseeds support hormone balance and reduce inflammatory pathways.
- Lean Proteins: Chicken, turkey, fish, tofu, and legumes — essential for blood sugar regulation and hormonal balance.
- Cruciferous Vegetables: Broccoli, cauliflower, Brussels sprouts, and cabbage contain Indole-3-Carbinol (I3C), which helps metabolize excess estrogen and may reduce cyst risk.
- Antioxidant-Rich Fruits & Vegetables: Berries, spinach, kale, and bell peppers fight oxidative stress linked to ovarian dysfunction.
Foods to Avoid with Ovarian Cysts
Foods That Worsen Ovarian Cysts
- Refined Sugar & Sweets: Cause insulin spikes, worsen androgen excess, and trigger cyst formation — especially harmful for women with PCOS.
- Red Meat & Processed Meats: Associated with a 2.7x higher risk of seromucinous ovarian cysts in research studies.
- Deep-Fried & Fast Foods: Trans fats increase inflammation and worsen insulin sensitivity.
- High-Fat Dairy: May disrupt hormone metabolism in some women; consider switching to low-fat or plant-based alternatives.
- Alcohol & Excessive Caffeine: Alcohol disrupts hormonal balance; excess caffeine contributes to inflammation and dehydration.
7-Day Ovarian Cyst Diet Plan Sample
Sample Weekly Diet Framework for Ovarian Health
- Monday: Oatmeal with berries + grilled salmon + quinoa salad with leafy greens
- Tuesday: Smoothie with flaxseed + turmeric lentil soup + stir-fried tofu with broccoli
- Wednesday: Greek yogurt with nuts + chicken breast + roasted cauliflower and brown rice
- Thursday: Eggs with spinach + mackerel + avocado salad with olive oil dressing
- Friday: Whole grain toast with almond butter + vegetable curry with lentils + mixed berry bowl
- Saturday: Overnight oats with chia + grilled turkey + Brussels sprouts with garlic and olive oil
- Sunday: Ginger herbal tea + vegetable soup with beans + baked fish with steamed vegetables
Ovarian Cyst Home Remedies — Natural Approaches to Ease Symptoms
While home remedies cannot shrink or eliminate ovarian cysts — and should never replace medical evaluation — several evidence-informed natural approaches can meaningfully reduce symptom burden, support hormonal balance, and complement medical treatment. These are the most searched natural remedies for ovarian cysts:
Important: Home remedies manage symptoms — they do not treat the underlying cyst. Always get a proper diagnosis first.
1. Heat Therapy
Applying a warm heating pad or hot water bottle to the lower abdomen for 15–20 minutes is one of the most effective and widely recommended approaches for relieving ovarian cyst pain. Heat relaxes the pelvic muscles, reduces cramping, and improves blood circulation to the pelvic region. Use a cloth barrier between the heat source and skin to prevent burns.
2. Anti-Inflammatory Herbal Teas
Several herbal teas with anti-inflammatory properties are traditionally used to support hormonal balance and reduce pelvic discomfort:
- Chamomile tea: Has mild anti-inflammatory and antispasmodic properties; helps reduce cramping.
- Ginger tea: A potent anti-inflammatory that can reduce pain and nausea associated with ovarian cysts.
- Spearmint tea: Some evidence suggests it lowers androgen levels, potentially beneficial for PCOS-related cysts.
- Turmeric (golden milk): Curcumin in turmeric has well-documented anti-inflammatory properties.
Note: Herbal teas are safe adjuncts for most women but should be discussed with your doctor during pregnancy.
3. Magnesium Supplementation
Magnesium plays a critical role in regulating insulin sensitivity and reducing inflammation — two key drivers of ovarian cyst formation, particularly in women with PCOS. Foods rich in magnesium include dark chocolate (70%+), almonds, spinach, and black beans. Supplementation (200–400 mg/day) may help reduce cramping and support hormonal balance, but should be discussed with a healthcare provider.
4. Castor Oil Packs (Traditional Remedy)
Castor oil packs — applying castor oil to the lower abdomen covered with a warm cloth — are a traditional naturopathic remedy used for decades to reduce pelvic inflammation and support lymphatic circulation. While robust clinical trial evidence is limited, many women report symptom relief. Do not use during pregnancy or when trying to conceive.
5. Stress Reduction Practices
Chronic stress disrupts the hypothalamic-pituitary-ovarian axis, leading to irregular ovulation and creating conditions favorable for cyst formation. The following practices have evidence for lowering cortisol and supporting ovarian function:
- Yoga — particularly restorative and yin yoga styles targeting the pelvis
- Meditation and mindfulness — even 10 minutes daily reduces cortisol significantly
- Deep diaphragmatic breathing exercises
- Progressive muscle relaxation — especially effective for pelvic pain management
6. Regular Moderate Exercise
Exercise is one of the most powerful lifestyle interventions for ovarian health. Moderate physical activity (150 minutes per week) reduces insulin resistance, lowers body weight, balances estrogen and progesterone, and reduces inflammation. The best types for women with ovarian cysts:
- Walking: Low impact, sustainable, and effective
- Swimming: Zero impact, excellent for pelvic pain
- Yoga and Pilates: Support core stability and hormone balance
- Avoid: High-impact twisting movements, heavy lifting, and intense HIIT if cysts are large
7. Omega-3 Fatty Acids
Omega-3 supplements (fish oil, algae oil) help manage the hormonal imbalances caused by ovarian cysts, reduce inflammation, and may help reduce androgen levels in PCOS. A typical therapeutic dose is 1,000–2,000 mg of combined EPA/DHA daily. Food sources include salmon, mackerel, sardines, walnuts, and flaxseeds.
8. Maintain Healthy Blood Sugar Levels
Because insulin resistance is one of the primary drivers of functional cysts and PCOS-related cysts, maintaining stable blood sugar is a powerful home strategy. Practical steps include:
- Eat every 3–4 hours to prevent blood sugar crashes
- Always pair carbohydrates with protein or healthy fat
- Avoid eating large amounts of carbohydrates alone (especially refined)
- Consider adding cinnamon to meals — studies show it improves insulin sensitivity
When Home Remedies Are NOT Enough — See a Doctor If:
• You have severe or sudden pelvic pain that is not relieved by over-the-counter painkillers
• You are pregnant and experiencing abdominal pain
• You have fever, vomiting, or signs of shock alongside pelvic pain
• Your symptoms are not improving after 2–3 menstrual cycles of watchful waiting
How to Prevent Ovarian Cysts Naturally — Complete Prevention Guide
While some ovarian cysts are beyond prevention — particularly those driven by genetics or medication — many risk factors can be meaningfully reduced through proactive lifestyle choices:
Dietary Prevention
- Follow a Mediterranean-style diet rich in vegetables, whole grains, olive oil, fish, and legumes.
- Reduce or eliminate refined sugars and processed carbohydrates.
- Maintain a healthy BMI — women with functional ovarian cysts tend to have higher BMI, and weight management significantly improves reproductive function.
- Eat cruciferous vegetables several times per week for natural estrogen modulation.
- Stay well hydrated with water and herbal teas rather than sugary drinks.
Lifestyle Prevention
- Exercise regularly: 150 minutes per week of moderate activity balances hormones, reduces insulin resistance, and supports a healthy BMI.
- Manage chronic stress through yoga, meditation, deep breathing, and mindfulness.
- Prioritize quality sleep (7–9 hours): Sleep regulates estrogen, progesterone, and melatonin — all critical for ovarian health.
- Avoid smoking: Linked to poor reproductive outcomes and oxidative stress.
- Limit alcohol: Even moderate consumption can disrupt estrogen balance over time.
- Reduce plastic exposure: Avoid heating food in plastic containers and choose glass or stainless steel.
Medical Prevention
- Schedule annual gynecological checkups including pelvic exams — early detection changes outcomes.
- Request a transvaginal ultrasound if you have irregular periods, pelvic pain, or a family history of ovarian cysts or cancer.
- Discuss oral contraceptives with your doctor if you have recurrent functional cysts.
- If undergoing IVF or ovulation induction, ensure close monitoring for ovarian hyperstimulation syndrome (OHSS).
- Know your family history: PCOS and certain ovarian cyst types have a genetic component.
Precautions for Pregnant Women with Ovarian Cysts
If you have been diagnosed with an ovarian cyst during pregnancy, here is what you and your care team should do:
- Establish baseline ultrasound measurements at diagnosis to track cyst changes.
- Schedule repeat ultrasounds every 4–6 weeks throughout the pregnancy.
- Know the warning signs of complications: sudden severe abdominal pain, nausea, vomiting, or fever — seek emergency care immediately.
- Avoid strenuous physical activities or sports that may increase the risk of ovarian torsion.
- Discuss your delivery plan with your OB-GYN — your cyst size and position will influence whether vaginal delivery or C-section is safer.
- If surgical removal is needed, advocate for second-trimester timing (weeks 14–20) for the lowest fetal risk.
- Do not ignore the cyst hoping it will disappear — most will, but those that don’t require timely decisions.
Ovarian Cyst vs PCOS — Key Differences Every Woman Must Know
One of the most common points of confusion for women is the difference between a simple ovarian cyst and Polycystic Ovary Syndrome (PCOS). They are frequently conflated but are very different conditions:
Ovarian Cyst vs PCOS — Side-by-Side Comparison
FEATURE OVARIAN WATER CYST PCOS
- Nature: Single fluid-filled sac vs. Multiple small follicles on both ovaries
- Hormones: Usually normal vs. Androgen excess (elevated testosterone/DHEA)
- Periods: May be temporarily irregular vs. Chronically irregular or absent
- Resolution: Often resolves on its own vs. Requires long-term management
- Fertility: Rarely affected vs. Commonly affected due to ovulation disruption
- Metabolic: No systemic effects vs. Insulin resistance, weight gain, diabetes risk
- Treatment: Watchful waiting / one-time surgery vs. Lifelong hormonal + metabolic management
The key takeaway: Having an ovarian cyst does NOT mean you have PCOS. However, women with PCOS are prone to developing multiple ovarian follicles that resemble cysts on ultrasound. A proper diagnosis by a gynecologist using ultrasound AND blood hormone levels is essential to distinguish the two.
Frequently Asked Questions (FAQs)
Q: Can an ovarian cyst go away on its own?
A: Yes — the majority of functional cysts (follicular and corpus luteum) resolve naturally within 1–3 menstrual cycles without any treatment. However, larger, complex, or persistent cysts require medical management.
Q: Is an ovarian cyst dangerous during pregnancy?
A: Most are not. Simple, small cysts discovered during pregnancy are typically monitored conservatively. However, large (>5–6 cm), persistent, or symptomatic cysts can lead to torsion, rupture, obstructed labor, or fetal malpresentation — all requiring prompt medical attention.
Q: What is the difference between a water cyst and PCOS?
A: A water cyst is usually a single, fluid-filled sac that often resolves on its own. PCOS is a hormonal disorder with multiple small follicles on both ovaries, irregular periods, androgen excess, and metabolic abnormalities requiring long-term management.
Q: Can I exercise with an ovarian cyst?
A: Gentle exercise like walking, swimming, and yoga is generally safe and beneficial. However, high-impact sports, heavy lifting, and twisting movements should be avoided as they can increase the risk of ovarian torsion or cyst rupture.
Q: How is an ovarian cyst removed during pregnancy?
A: Laparoscopic cystectomy (keyhole surgery) during the second trimester (weeks 14–20) is the preferred approach when surgery is necessary. Open surgery may be required for very large cysts. In some cases, cystectomy is performed simultaneously with a planned Caesarean section.
Q: Does an ovarian cyst mean I have cancer?
A: Overwhelmingly, no. An IOTA5 study analysis found only 12 cases of ovarian cancer in 1,919 women with cysts — a 2-year cumulative cancer risk of just 0.4%. Simple cysts are not associated with increased cancer risk. Complex cysts or solid masses warrant further evaluation.
Q: What are the best home remedies for ovarian cyst pain?
A: Heat therapy (warm pad on the lower abdomen), ginger tea, chamomile tea, omega-3 supplementation, gentle yoga, and stress reduction techniques are the most evidence-supported home approaches. These manage symptoms but do not treat the cyst itself — medical evaluation remains essential.
Q: Can ovarian cysts cause miscarriage?
A: Most ovarian cysts do not cause miscarriage. However, large or complex cysts causing significant hormonal imbalances — particularly those related to PCOS or endometriosis — may increase miscarriage risk in some women. Regular monitoring during pregnancy is essential.
Conclusion: Your Ovarian Health Deserves Attention — Not Anxiety
Ovarian water cysts are incredibly common, often harmless, and frequently self-resolving. But when they persist, grow, or appear during pregnancy, they demand informed, proactive medical care. The good news is that with today’s diagnostic tools — especially early ultrasound screening — most cysts are caught and managed long before they become serious.
The most empowering thing any woman can do is stay informed, schedule regular gynecological checkups, eat a hormone-supportive diet, manage her weight and stress, use evidence-informed home remedies for symptom relief, and know the warning signs that require immediate medical attention.
Whether you are in your teens, your reproductive years, or approaching menopause — your ovaries work hard every cycle. Give them the care they deserve.
Are You Worried About Ovarian Cysts?
Get reliable medical information, symptom guides, and expert-reviewed health content all in one location.
For Reliable Health Information, Go to MedRankSEO.com
Regular updates · Expert-backed information · Free resources
| Medical Disclaimer: This article is intended for informational and educational purposes only. It does not constitute medical advice, diagnosis, or women’s health treatment. Always consult a qualified healthcare provider or gynecologist for personalized guidance regarding any medical condition. If you are experiencing severe pelvic pain or believe you have a ruptured cyst, seek emergency care immediately. |